


The information provided here is meant for newer CT technologists to the world of Cardiac CT. This basic overview is vendor neutral and includes some of the necessary building blocks that leads to high quality CCTA scans.
Recommended Building Blocks and Considerations
Patient BMI. The BMI is more accurate than simple body weight as it takes into consideration the height and weight of the patient. It is important to then note if the patient has more adipose tissue vs. muscle and overall chest mass. Consider separate protocols for BMI’s of </> 25.
Quality of IV. The type, size, quality of flow and placement of IV access is of paramount importance. This cannot be stressed enough! Once optimal placement of IV (including right AC vs. left, etc.) has been established, it should be HIGHLY considered that a test injection of saline be performed at least 1.0 ml/sec higher than selected contrast injection rate to offset the pressure from the viscosity difference of the saline and contrast injection.
Test injection should be performed with arms above the head in the scan position.
BD Diffusics needles recommended.
BD Nexiva™ Diffusics™ closed IV catheter system | BD
High injection rates and pre-warmed contrast. This will greatly affect both image quality and lower pressure limits. This will also help to reduce the chances of infiltration from lowered viscosity pressures. Higher injection rates due to faster scanners should also be considered. Contrast should be high osmolality, such as, Isovue 370, Omni 350, etc.
ECG placement and Patient Positioning. It is recommended that BEFORE placing ECG leads, the patient should be made as comfortable as possible, with arms ABOVE the head in a relaxed position. This may take an extra minute or two, however COMFORTABLE and CORRECT positioning will help to ensure REDUCED patient MOTION and increased ECG Tracing.
3M Red Dot Electrodes (with black connection posts) seem to work best (See supporting documents). *Keep in mind, many facilities no longer support the usage of razors or abrasive means for ECG prep.
Practice Breathing. Perform practice breath holds of 15 seconds or longer while at the scanner with the patient. The clearer the communication, expectations, and practice of prior breath holds, the greater the chances the patient will cooperate during the actual scan.
May need to create manual breath hold specific for CCTA scanning to allow for additional time prior to scan to allow for heart rate drop.
Manual Image Review. For CCTA scanning, it cannot be recommended enough for technologists to manually review initial CCTA images and then post-process accordingly and send appropriate images series. See above for more information regarding optimal CCTA workflow
Optimal Workflow (Basic)
This is extremely important for optimal image quality. Keep in mind, medications should be given in the sequence as per physician and protocol.
- Choose scan type – Axial Volume or Helical based on scan ordered (anatomy) and protocol.
- Determine BEST placement for radiation in the cardiac cycle depending upon rate, rhythm, etc.
- Scan patient
- Review the initial images to detect if any motion is present or other issues detected (such as: ECG tracing issues, breathing, cardiac, or patient motion).
- If motion is detected:
- Reconstruct additional phase or phases. Multiphase reconstruction may be performed if several phases are required for different segments of the coronary arteries to be motion free.
- The ECG should also be reviewed to ensure no miss-tagging of R-wave. Editing tags may be necessary.
- Send desired series to PACS, reading station, HeartFlow, Clearly, or other vendor analysis as needed or instructed.
Calcium Scoring
Scan Parameters
- 120 kV – keep scatter reduced from unknown calcium accumulation.
- Heart Rate up to 65: utilize 70-75% phase.
- Heart Rate above 65: utilize 40-45% phase
- If irregular rhythm is present, user can manually set a millisecond (ms) systolic scan range.
Coronary Evaluation Exams
- BMI below 25
- 80-100 kV may be utilized for CCTA exams.
- NO calcium on CA Score scan.
- NO stents.
- NO metal implants.
- Normal to small breast/chest mass.
- Contrast injection rates NO less than 5 to 6 ml/sec.
- 80-100 kV may be utilized for CCTA exams.
- BMI over 25 or known calcium, stents or bypass
- 120 kV recommended.
- 140 kV may be needed for significantly larger BMI’s. Follow physician-based protocols.
- Contrast injection rates no less than 6 ml/sec.
- 7 ml/sec. + may be required for significantly larger BMI’s. As before, follow physician-based protocols.
- 120 kV recommended.
Reminders
- Manual Settings (based upon physician oversite and protocols).
- Diastolic scanning – steady H.R. of generally 65-68 BPM or lower.
- Systolic scanning – irregular H.R. of generally 68 BPM or greater. May include a larger scan window (such as: 40-80%, etc.).
- If irregular rhythm is present, user can manually set a millisecond systolic scan range for more accuracy verses % scanning. *Highly recommend helical in this case.
- Cardiac breathing commands may need to be manually created if longer delay time required for H.R. to drop prior to scan (scanner dependent).
Pulmonary Vein, LVAD, & Other Cardiac Specialized Exams
- 120 kV as calcium, metal or prior surgeries with implanted devices is most common.
- 100 kV or lower may be utilized with confirmation of NO calcium, stents, metal, implanted devices, clips, etc. 140 kV may be needed for significantly larger BMI’s.
- Post LVAD will require a minimum of 120 to 140 kV due to excessive metal from implanted device.
- Contrast injection rates of no less than 5 to 7 ml/sec.
- Systolic scanning –35% to 45% range or manual millisecond from R-wave.
- Delayed scan – repeat cardiac scan at 60 – 90 seconds.
- Note: not all customers utilize this protocol.
- Follow protocols of overseeing physician.
TAVR
- Cardiac Scan
- Systolic scanning – 200-350 ms. scan range.
- 120 kV due to excessive calcium.
- Injection 4-6 ml/sec.
- CTA Chest, Abdomen, and Pelvis
- Scan a little above shoulders and a little below pelvis.
- Injection 4-6 ml/sec.
Bolus Tracking ROI Placement.
Bolus Tracking ROI should be placed in the descending aorta, away from calcium, scatter from superior vena cava (SVC), and movement of ascending aorta. The descending aorta is very stable in comparison to the cardiac movement of the ascending aorta.
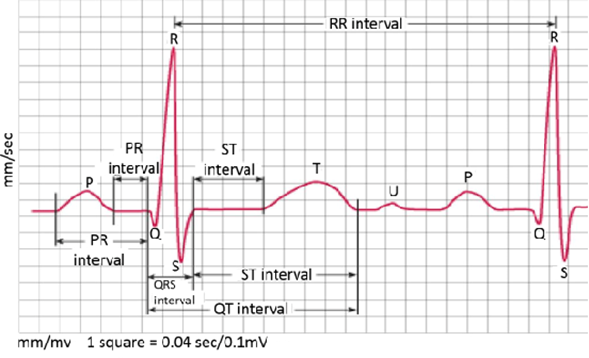
| Cardiac Cycle Review |
Review of basic ECG heart cycle wave form.
Systolic and diastolic scan range considerations
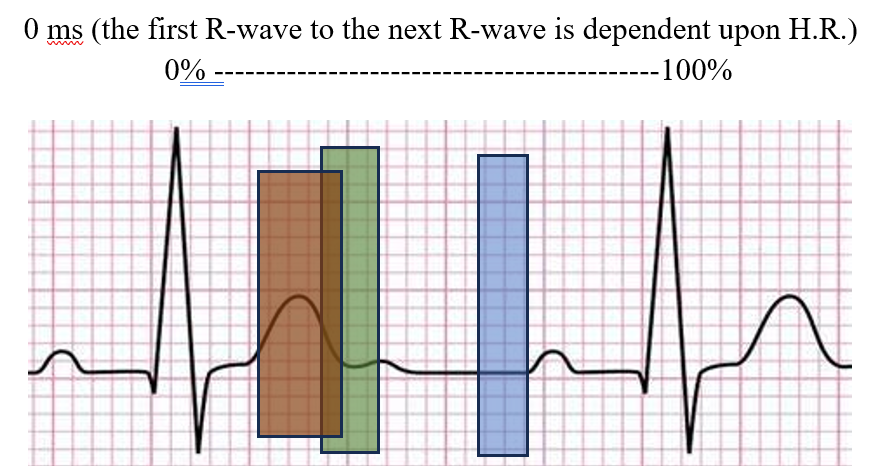
Graph above represents:
Coronary Arteries – Green (systolic [aka. sweet spot]) & Blue (diastolic)
Pulmonary Vein – Green (systolic)
TAVR Heart – Red (200-350 ms)
Systolic scanning has benefits for:
- High heart rates.
- Arrythmia (R to the T wave generally is stable in time)
- Filling of heart for TAVR, Pulmonary Vein, etc.
Basic Cardiac Anatomy
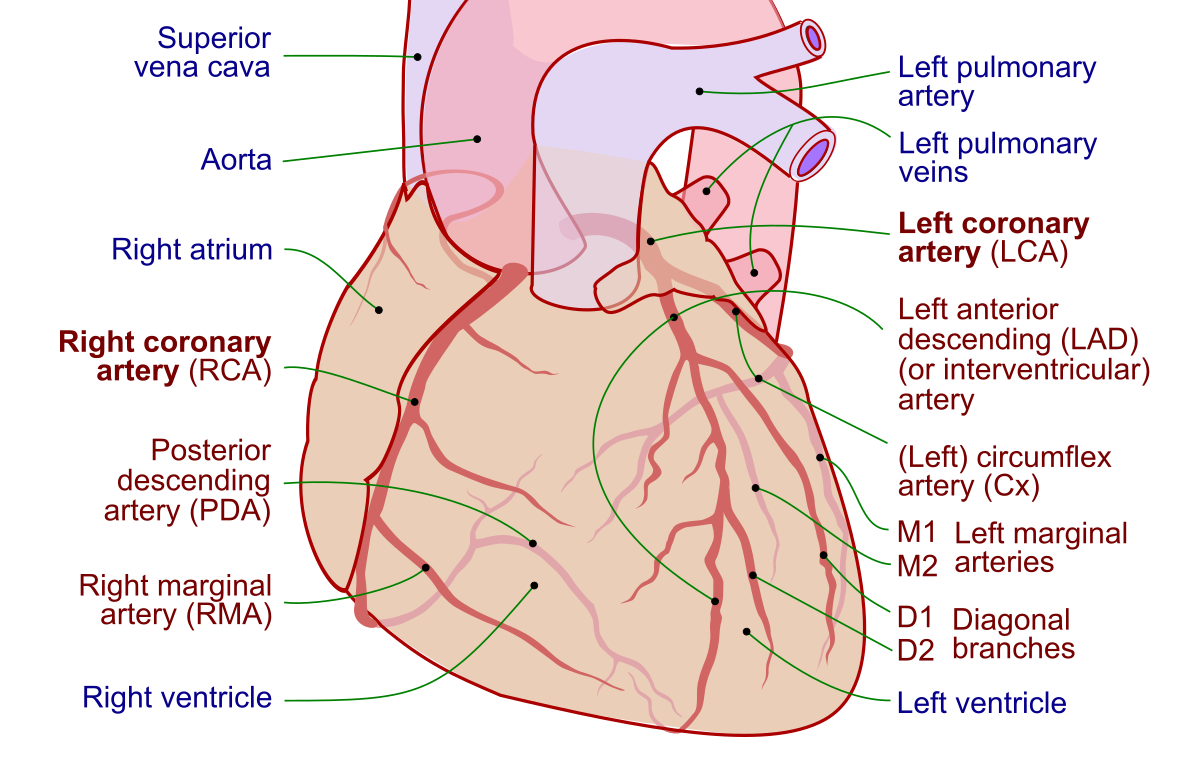
Visit the Society of Cardiovascular Computed Tomography (SCCT) for more information.
I cut my teeth as an EMT, CPR Instructor and Volunteer Fireman. From CT to applications, from lead to director, from sales and marketing to teaching, from general diagnostic to specialized Cardiac CTA, from patient care to PACS Administrator, from Travel Technologist to offering council for younger techs. – there is not much in this field I have not done. Along with all this, I have been a vendor at RSNA, NMSRT Conference speaker, interim didactic radiology physics instructor, and worked in well over more hospitals and clinics than most people have driven past. When requested, I also consult for new Radiology department builds and inner department corrective issues as requested.

Alongside healthcare I have written 15+ books, rebind old books and Bibles, speak itinerantly, and help to make aware the need and organizations who “hunt monsters” (human trafficking). And on a personal note, away from the lesser professional stuff, I love The Glenn Miller Orchestra and a fine cup of freshly roasted and ground coffee!

Leave a comment